Associação Portuguesa de Investigação em Cancro
Agressividade da displasia epitelial do estômago de tipo gástrico
Agressividade da displasia epitelial do estômago de tipo gástrico
Autores e afiliações:
Pedro Valente 1, Mónica Garrido 1, Irene Gullo 1,2, Helena Baldaia 3, Margarida Marques 3, Francisco Baldaque-Silva 3,4, Joanne Lopes , Fátima Carneiro 1,3,5
1 Faculty of Medicine of the University of Porto, Porto, Portugal
2 Faculty of Medicine and Surgery, Genova, Italy
3 Centro Hospitalar de São João, Porto, Portugal
4 Department of Gastroenterology and Hepatology, Karolinska University Hospital, Stockholm, Sweden
5 Institute of Molecular Pathology and Immunology of the University of Porto (IPATIMUP), Porto, Portugal
Abstract:
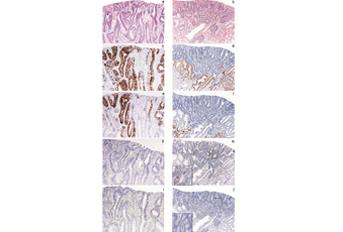
Abstract Background: Gastric dysplasia is classified as adenomatous/type I (intestinal phenotype) and foveolar or pyloric/type II (gastric phenotype) according to morphological (architectural and cytological) features. The immunophenotypic classification of dysplasia, based on the expression of mucins, CD10 and CDX2, recognizes the following immunophenotypes: intestinal (MUC2, CD10 and CDX2); gastric (MUC5AC and/or MUC6, absent of CD10 and absent or low expression of CDX2); hybrid (gastric and intestinal markers) and null. Methods: Sixty-six cases of non-polypoid epithelial dysplasia of the stomach were classified according to morphological features (histotype and grade) and immunophenotype. Immunohistochemical staining was performed with antibodies against MUC2, MUC5AC, MUC6, CD10, CDX2, chromogranin, synaptophysin, Ki-67 and TP53. HER2 alterations were analysed by immunohistochemistry and silver-enhanced in situ hybridization (SISH). Results: By conventional histology, dysplasia was classified as adenomatous/intestinal (n=42; 64%) and foveolar or pyloric/gastric (n=24; 36%) and graded as low-grade (n=37; 56%) and high-grade (n=29; 44%). Immunophenotypic classification showed intestinal (n=22; 33.3%), gastric (n=25; 37.9%), hybrid (n=17; 25.8%) or null (n=2; 3.0%) phenotypes. In 20 cases a coexistent intramucosal carcinoma was identified. The intestinal immunophenotype was shown to be significantly associated with low-grade dysplasia (p=0.001), high expression of CDX2 (p=0.015), TP53 (p=0.034), synaptophysin (p=0.003) and chromogranin (p<0.0001); the gastric immunophenotype was significantly associated with high-grade dysplasia (p=0.001), high Ki-67 proliferative index (p=0.05) and coexistence of intramucosal carcinoma (p=0.013). HER2 amplification was observed in 3 cases, typed as gastric or hybrid. Conclusions: Epithelial non-polypoid dysplasia of the stomach with gastric immunophenotype shows features of biological aggressiveness and may represent the putative precursor lesion in a pathway of gastric carcinogenesis originated de novo from the native gastric mucosa, leading to gastric type adenocarcinoma.
Revista: Gastric Cancer
http://link.springer.com/article/10.1007%2Fs10120-014-0416-5

